

IDD Citizens are losing their CLS caregivers as the county transitions to the CCBHC model of Socialized Health Care
Ottawa County and counties across the country are in the process of establishing Certified Community Behavioral Health Centers (CCBHC). A CCBHC is not a physical building but rather a collection of private, non-profit, and government health care service centers working together and usually receiving funding through one of the various state or federally run CCBHC programs. This new model is transforming the health care system in ways that may not be desired by residents.
For example, people with Intellectual and Developmental Disabilities (IDD) are not eligible for Certified Community Behavioral Health Center (CCBHC) services unless they have a dual diagnosis (both an Intellectual and Developmental Disability and a mental illness or substance use disorder), but once they have a dual diagnosis and receive CCBHC services, they are no longer eligible for other services which enable them to live as normal lives within the community as possible. CCBHC services are for people with both mental illness and substance use disorder (SUD), not IDD. This is because IDD conditions such as autism (ASD) and Down’s Syndrome do not change with medication or psychological treatments. Rather, it is assistance with routine activities (such as getting dressed) and getting out into the community from community living support (CLS) caregivers that enable IDD people to live as normally as possible.
People with IDD do best when living at home or in small group settings in conjunction with community living supports which are paid for through the Home and Community-Based Support 1915 (c) programs. Through these programs people with IDD can receive non-mental health alternative services such as music therapy, massage therapy, art therapy, recreational therapy, and speech and occupational therapy. If people with IDD are given a dual diagnosis and begin to receive care under the CCBHC model, they cruelly are no longer eligible for community living support services (CLS). The same is true if an IDD patient is misdiagnosed as someone with mental illness or SUD. For example, autism is characterized by a combination of social and/or communication disabilities with repetitive, ritualistic behaviors. If only these characteristics are considered, they could be diagnosed with schizophrenia, mood disorder, or even bad parenting. The consequences can be devastating for the IDD patient.
Unfortunately, it is extremely easy for people with IDD to be given dual diagnoses. For example, if they are prescribed a medication to help with sleep that happens to be addictive, and that medication is suddenly removed, they now qualify as someone with a substance use disorder (SUD) and can be treated under CCBHC. Likewise, if a teenage IDD female experiencing premenstrual syndrome is prescribed medication to help control moods, removal of that medication could result in withdrawal and a SUD diagnosis. If an individual with IDD, living in a group home, is having difficulty communicating and acts out physically, they could be given a behavior diagnosis and placed on medication. Not providing devices that aid in communication increases this likelihood. Once an IDD individual receives a dual diagnosis and begins receiving services under the CCBHC model, it can put them at grave risk for abuse and exploitation because they lose their community living supports (CLS).
Dual diagnosis tends to force people with IDD into institutional living situations. Since the CCBHC model does not contain provisions for community living support services, this leaves social recreational programs, such as those offered by the Momentum Center, and reliance on friends and family members who are willing to bring them places, as their primary options for getting out into the community.
Prior to 2015, Kandu Industries operated in Ottawa County. It was a program supported by Medicaid that provided job training for meaningful work for people with intellectual and developmental disabilities (IDD). It was started by parents of IDD children, and fulfilled a great need, as it helped to integrate people with IDD into the community. CMHOC board notes from November 2016 show that when Kandu was forced out of business, social recreational programs were created to replace the void.

A complicating factor is that many people with IDD are placed into group homes located physically far away from loved ones. Although loved ones can request placement in particular homes, and even find desirable places for their loved ones near to home, CMHOC has no obligation to accommodate the requests. In Ottawa County, approximately 50% of CMHOC Adult Foster Care recipients are placed in homes outside of the county. These situations are particularly hard on families. Rather than regularly visiting their loved ones during lunch breaks and after work, when they are placed over an hour’s drive away, visits become limited to weekends and holidays. The resulting decrease in community interaction, increases the chances these IDD consumers will act out, and thereby receive a dual diagnosis.
Not only are IDD people at a high risk for being institutionalized, they are at risk of being confined in prison as well. The introduction of radical sexuality education for people with IDD increases the risk that they will act sexually inappropriate in public. This could result in arrest and imprisonment.
Some community members are catching onto what is happening to their loved ones and are beginning to ask questions. During the July 24, 2023, Community Mental Health board meeting, a local resident gave the following public comment.
(2:31:34)
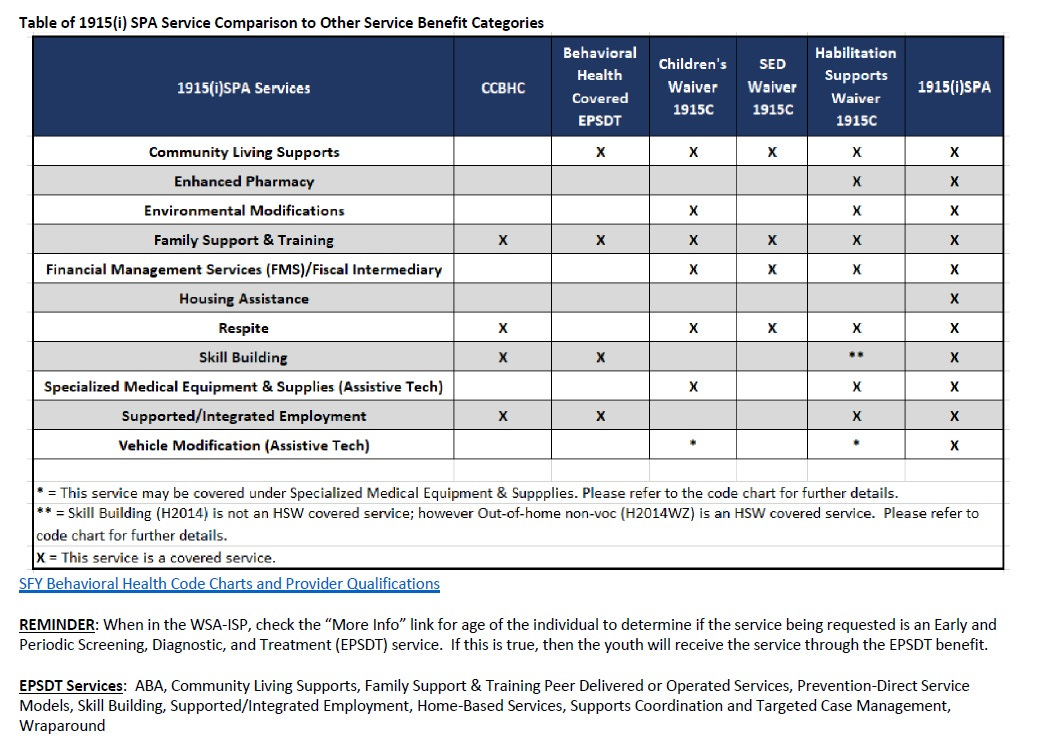
“I am requesting a presentation on the 1915I state plan Amendment plan, because several people are not being allowed to be enrolled in this plan. This plan also provides for housing. [] So, I FOIAed the specialized residential applications, and apparently, the gaps and services are because CMH, in some situations, have taken away home and community-based community living supports (CLS) services from people in adult foster care homes, and then they have no alternatives, but to then go into a CCBHC social recreation program where data collection is being taken for their CCBHC health care reform initiative.
So, I am begging the board to please look into that, because if services are being taken away from people, and they're being left with no recourse but to go to Momentum [Center] or other social programs, I don't think that that is the right thing to do. I think it's a conflict of interest. [] So what that means is the reason why CMH is pushing back on conflict-free case management, is that if people are given the power to choose their services, then there's no need for case managers.”
Listen closely at the end. She must have been right on target, because the board president immediately said, “cut her off” when her time was up. Why wouldn’t the board want to look into these concerns?